The cornea is the thin transparent tissue covering the front of the eye. The inner layer of cells, consisting of endothelial cells, are responsible for pumping fluid out of the cornea. In effect, this endothelial layer helps to keep the cornea crystal clear. Unfortunately, the endothelium does not regenerate. You are born with these cells and they do not grow back when they are damaged.
In certain eye conditions such as Fuch’s dystrophy and bullous keratopathy, the endothelial cells no longer function and this causes the cornea to swell and vision deteriorates as the cornea begins to cloud.
The usual thickness of the entire cornea is ~540 microns. When the endothelial cells are not pumping well, the cornea can swell to the 600-1000 micron range. The cornea is no longer clear when it is swollen because the collagen fibers are no longer able to remain parallel. At this point, the corneal dysfunction can usually be treated medically with saline eyedrops (Muro 128 Solution 5%, Bausch & Lomb or Sochlor 5% solution, OCuSOFT).
Swelling in the cornea, called corneal edema, can worsen to the point where blisters form in the cornea. These blisters can erupt causing painful bullae. This condition is called bullous keratopathy. Bullous means blisters and keratopathy means a disease of the cornea. At the point where the corneal swelling is no longer well controlled with medical therapy, we can turn to surgical treatments like DMEK.
How does the DMEK transplant work to keep the cornea clear?

Descemet membrane endothelial keratoplasty (DMEK) is a type of partial thickness corneal transplant surgery. In this surgery, only the endothelial cell layer containing the endothelial cells are transplanted. The endothelial cells pump out fluid and keep the cornea clear.
The DMEK procedure involves the following steps:
- Donor Graft Preparation: A thin layer of tissue containing the Descemet’s membrane and healthy endothelial cells is harvested from a donor cornea. Now in 2023, the grafts are usually preloaded in a glass cartridge called Jones Tube by the Eye Bank in preparation for the surgery.
- Patient’s Cornea Preparation: The patient’s cornea is prepared by creating a small incision or manually peeling off the damaged Descemet’s membrane and endothelial cells.
- Donor Graft Insertion: The prepared donor graft is delicately unfolded and placed onto the patient’s cornea, with the Descemet’s membrane and healthy endothelial cells facing the patient’s eye.
- Graft Adherence: An air or gas bubble is typically injected into the eye to help secure the graft in place against the patient’s cornea. The patient may be positioned in a specific manner to ensure optimal graft adhesion.
In summary, during a DMEK corneal transplant, your cornea surgeon will remove the damaged corneal cells, unscroll the donor graft, and then replace the thin graft layer containing healthy endothelial cells which will pump the cornea clear and compact.
What is the difference between DSEK and DMEK?
DSEK/DSAEK: This is a partial thickness transplant including posterior stroma along with with descemet’s membrane and endothelial cells. This is a thicker transplant.
DMEK: This is the thinnest corneal transplant including descemet’s membrane and endothelial cells.
Compared to other types of corneal transplantation, such as penetrating keratoplasty (PK) or Descemet’s stripping automated endothelial keratoplasty (DSAEK), DMEK offers potential advantages including better visual outcomes, faster recovery, and reduced risk of complications like graft rejection and induced astigmatism.
What is aftercare and recovery time like?
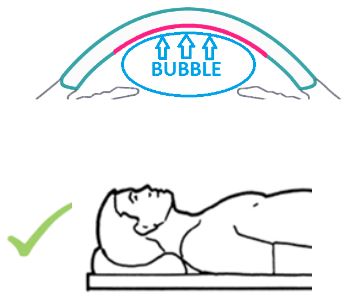
The DMEK graft is held into place with an air bubble which is placed in the eye. During the first 24 hours after surgery, position on our back facing upwards. Limit time upright to short trips to the bathroom and eating. Avoid looking downwards as that can cause the graft to detach and dislocate which requires additional procedures to reattach.
Your vision will be extremely blurry the first few days because the air bubble covering the graft will block out your vision. During the first few days, your surgeon may advise you to continue positioning on your back for several hours each day and to sleep directly on your backwards lookup at the ceiling. As the air bubble reabsorbs, you will notice a line in your vision. The bottom portion of your vision will be very blurry and the top portion will start to clear. As the bubble becomes smaller and smaller, you may notice it dance around as you walk or move from lying to standing.
Avoid rubbing or touching your eyes. Follow all post-operative instructions which usually include a series of drops and sometimes ointments. Typically, your surgeon will want to see you the day after surgery and within the first week of surgery. Typically, vision recovers by 2-4 weeks following surgery.
In 10-15% of DMEK surgeries, it may be necessary to have some additional air placed in the eye in a rebubble procedure. During this procedure, your surgeon places more air into the eye to allow the corneal graft to completely attach. DMEK surgery can occur prior to cataract surgery, after cataract surgery or concurrently with cataract surgery depending on your eyes and your surgeon’s preference.
This article was originally written on 2/10/2022 by Angelique Pillar, MD and updated on 5/28/23.